Ulnar Nerve Subluxation
- The ulnar nerve or “funny bone” nerve is one of three main nerves in your arm. It travels behind the inside part of the elbow and compression or irritation of the nerve can cause numbness and tingling into the small and ring finer of the hand
- The throwing motion with elbow flexion greater than 90 degrees combined with rapid acceleration has been shown to place significant strain on the ulnar nerve
- This can lead to compression of the nerve and in some cases instability of the nerve. Instability typically presents with “popping” or “snapping” of the nerve during the throwing motion. This can lead to numbness, tingling, pain as well as difficulty with control and velocity while throwing
SYMPTOMS:
- In the overhead athlete, ulnar nerve compression and instability are both often a dynamic phenomenon, therefore these athletes will complain of paresthesia’s (numbness or tingling) during the throwing motion but not necessarily at rest
DIAGNOSIS:
- The upper extremity should be examined for additional pathology including cervical radiculopathy, thoracic outlet syndrome, ulnar tunnel syndrome at the wrist, medial epicondylitis, elbow arthritis, UCL insufficiency and carpal tunnel syndrome
- Radiographs should be obtained to evaluate for bony abnormalities
- Advanced imaging such as MRI or US as well as electrodiagnostic testing is not routinely necessary although it can aid in diagnosis
TREATMENT:
- Nonoperative treatment includes postural modification to avoid positions of elbow flexion and direct pressure as well as physical therapy for scapular stabilization
- Given the significant strain placed on the ulnar nerve and increased anterior translation of the nerve in the throwing athlete, surgical treatment is the preferred treatment for cubital tunnel syndrome or ulnar nerve hypermobility in the throwing athlete
- Surgical treatment consists of an ulnar nerve transposition or “moving” of the ulnar nerve so that is no longer compressed or unstable

POSTOP:
- Postoperatively patients are placed in soft dressing to allow for immediate ROM to maintain excursion of the nerve and prevent scarring at the site of transposition
- Occupational and physical therapy can aid in additional stretching and strengthening
- Majority of throwing athletes have return to full activity by 12-14 weeks
ACONEUS EPITROCHLEARIS:
- The anconeus epitrochlearis (AE) is an anomalous accessory muscle along the medial elbow that can be an uncommon cause of ulnar nerve compression
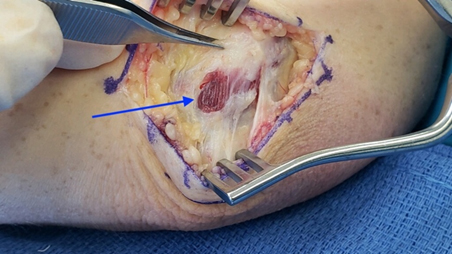
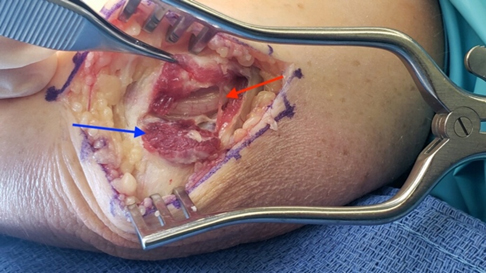
Hypertrophic anconeus epitrochlearis is found at the time of ulnar nerve decompression in a 34 y/o professional baseball player with ulnar nerve symptoms (Blue Arrow = AE; Red Arrow = Ulnar Nerve)
REVISION ULNAR NERVE SURGERY:
- Occasionally an athlete will undergo elbow surgery or ulnar nerve release and have ongoing ulnar nerve symptoms
- Typically, they will have persistent numbness within the small and ring finger or present with vague, ill-defined pain along the medial elbow that worsens with physical activity
- Persistent symptoms can be secondary to subluxation of the ulnar nerve or in some cases the nerve can become entrapped or compressed within scar tissue
- Patients who have worsening of ulnar nerve symptoms or symptoms that fail to improve clinically over a reasonable amount of time should be considered for revision surgery
- Revision surgery typically consists of ulnar nerve transposition utilizing a variety of methods to transpose and secure the nerve in bed of tissue that will reduce the possibility of scarring around the ulnar nerve
CASE EXAMPLE:
- This 22 y/o collegiate pitcher who underwent ulnar collateral ligament reconstruction surgery by an outside physician 6 months prior and was referred for worsening elbow pain and numbness
- At the time of his UCL reconstruction he underwent an ulnar nerve transposition utilizing a fascial sling from the intermuscular septum
- He describes ongoing pain and vague discomfort to the anteromedial aspect of his elbow and numbness to the ring and small finger that worsens during physical therapy
- Physical exam demonstrates stability along the medial elbow with no pain along the course of the ligamentous reconstruction. His exam is reassuring for ligamentous stability. His pain is specifically anterior to the medial epicondyle
- Physical exam demonstrates irritability of the ulnar nerve along its course and pain with full elbow extension

Patient localizes pain along the course of the green markings just anterior to the medial epicondyle
- After failing to improve over a reasonable amount of time and worsening neurologic symptoms with physical activity, the decision was made to pursue revision ulnar nerve surgery
- At the time of his surgery, the ulnar nerve was found to be scarred and entrapped along the medial epicondyle where the fascial sling had been sewn
- The nerve was released and transposed anteriorly utilizing a subfascial intramuscular approach to ensure the nerve was free of any entrapment
- Postoperatively the patient began early ROM to minimize scarring and ultimately returned to play free of neurologic symptoms
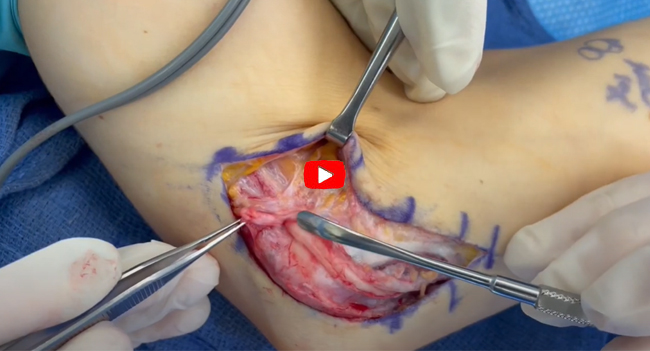
Previously transposed ulnar nerve is found adhered to the medial epicondyle and fascial sling
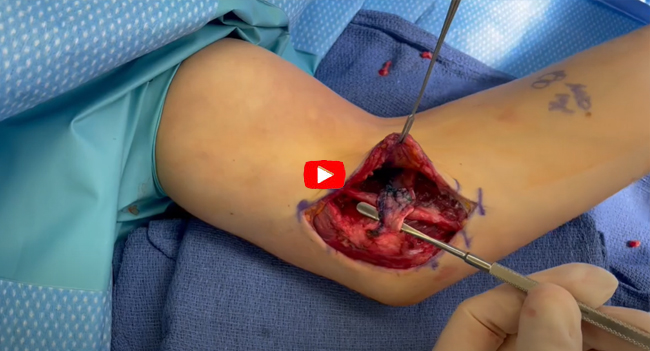
Ulnar nerve is dissected free from surrounding scar tissue
In revision scenarios the ulnar nerve is commonly transposed anteriorly within the muscle layer